心筋症診断における心臓MRI T1 mappingとECV解析 ― LGEに代わるイメージングモダリティの幕開け 第2回 Cardiovascular Imaging Symposium
投稿日:(医療法人豊智会、バイエル薬品株式会社共催)
「心臓MRIのT1 mappingおよびECV解析について」に関する発表抄録掲載
去る平成30年10月17日、医療法人豊智会はバイエル薬品の協賛・共催で「第2回Cardiovascular Imaging Symposium」を東京白金台八芳園にて開催致しました。盛会のうちに終了できましたことをご報告致します。
循環器内科科長の手塚が当院における3T心臓MRI(Siemens社)によるT1 mappingとECV解析のデータを発表致しましたので、下記に発表スライドの一部と抄録を掲載させていただきます。
【発表抄録】
「心筋症診断における心臓MRI T1 mappingとECV解析」
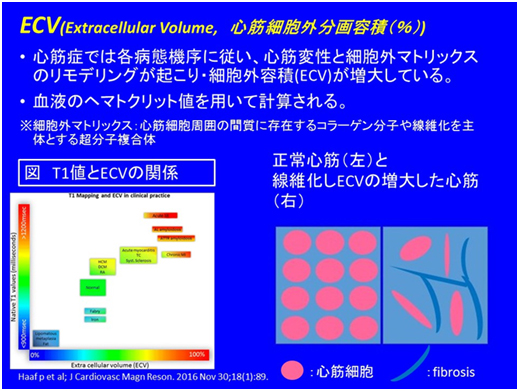
背景: 心臓MRIによる遅延造影検査は心筋線維化を描出し、その後の心イベントの発症と相関することから、心筋症での患者予後層別化の因子となり得る。しかし拡張型心筋症ではinversion timeの設定の困難もあいまって、4割ほどしかLGE陽性とならない。新しい撮像法であるT1 mappingではT1値を定量化するとともにECVを算出することができる。
方法: 全30症例で心臓MRI(T2WIBB、シネ、T1 mapping、遅延造影検査)が施行され、解析対象とした。心エコーのデータもさらに検討し、EF値(%)と左室拡張末期径(LVDd(mm))が記録された。拡張型心筋症は臨床的に診断されたものを対象とした。コントロールは正常左室壁運動をもつものと定義された。左室心筋のAHA16分類の各部位で計測したECVをセグメンタルECV(ECVsegと定義し、解析した。
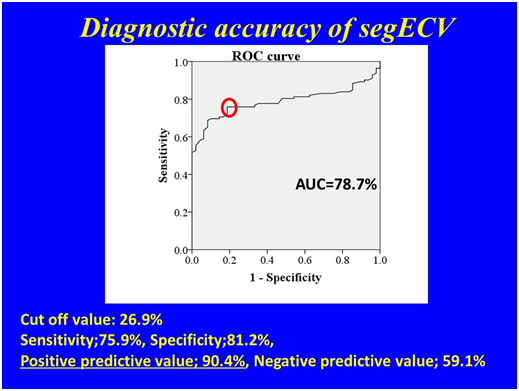
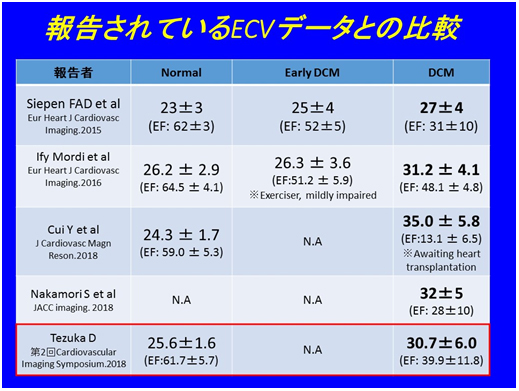
結果: 拡張型心筋症は7例、コントロールは3例で解析した。拡張型心筋症の症例のEFはコントロールと比較して有意に低かった(39.9±11.8 v.s 61.7±5.7%, p=0.005). また拡張型心筋症の症例の左室拡張末期径(LVDd)は有意に高かった(60.7±7.8 v.s 47.3±2.1, p=0.003)。 拡張型心筋症のECVseg(n=112) はコントロール(n=36)と比較して有意に高かった (30.7±6.0 v.s 25.6±1.6%, p<0.001)。拡張型心筋症を診断するROCカーブの解析ではカットオフ値26.9%によりAUCが78.7%であった。ECVsegの診断精度を求めたところ感度75.9%、特異度81.2%、陽性的中率90.4% 、陰性的中率59.1%であった。
結論: ECVsegは拡張型心筋症の検出に有用であった。
【Abstract】
Diagnostic Ability of myocardial T1 Mapping and Extracellular Volume Fraction Analysis used by Cardiac Magnetic Resonance Imaging in patients with Dilated Cardiomyopathy
Daisuke TezukaMD.PhD.1
Department of Cardiovascular Medicine, Advanced Imaging Center Yaesu Clinic.
Introduction: Cardiac Magnetic Resonance (CMR) imaging used by late gadolinium enhancement (LGE) can detect myocardial fibrosis, which correlated with future cardiac adverse event, and become an indicator for stratifying outcome of patients with cardiomyopathy. However, in cases with dilated cardiomyopathy (DCM), LGE can be detected in the 40% cases of DCM due to the difficulty of setting inversion time by the examination. New imaging modality, myocardial T1 mapping quantifies native T1 value and can calculate extracellular volume fraction (ECV).
Methods: A total 30 cases underwent complete evaluation with CMR (T2 weighted image block blood, T1 mapping with and without enhancement, and LGE study) in our clinic, and the whole data was reviewed. The data of echocardiography was checked in the all cases. Ejection fraction (EF(%)) and left ventricular end-diastolic diameter (LVDd(mm)) was recorded by the echocardiography or the CMR cine imaging. The patients with DCM were defined as having its clinical diagnosis in their hospitals. Control case was defined as normal LV function by cine imaging. Segmental ECV (ECVseg) was calculated in the AHA 16 segments of LV by setting ROI in the each lesion.
Results: The number of DCM patients was 7 cases. EF in DCM cases was significantly lower than the control cases (39.9±11.8 v.s 61.7±5.7%, p=0.005). LVDd in DCM cases was higher than the control cases (60.7±7.8 v.s 47.3±2.1mm, p=0.003). ECVseg of DCM (n=112) was significantly higher than that of control cases (n=36) (30.7±6.0 v.s 25.6±1.6%, p<0.001). The ROC curve demonstrated 78.7% of AUC when cut off value was 26.9%. The diagnostic accuracy of ECVseg was 75.9% of sensitivity, 81.2% of the specificity, 90.4% of the positive predictive value, and 59.1% of the negative predictive value.
Conclusion: Segmental ECV analysis by T1 mapping of CMR was useful for the detection of DCM cases.
- わかっていてもできないダイエット ―食事療法はどうやるか― 連載第六回目 - 2022年7月5日
- わかっていてもできないダイエット ―まずは朝の体重計測が基本―連載第五回目 - 2022年1月7日
- わかっていてもできないダイエット ―ダイエットでお金がたまる?―連載第四回目 - 2021年10月4日